Clinical symptoms, such as sore throat, fatigue, headache, etc, can be associated with both Lyme disease and infectious mononucleosis. But, there lies a major difference between the two conditions. Lyme disease is a bacterial infection (caused by Borrelia burgdorferi), whereas infectious mononucleosis is a viral infection (caused by Epstein Barr virus).
Sometimes, both the infections can coexist in an individual. In this blog, we will discuss the overlapping clinical symptoms of Lyme disease and infectious mononucleosis.
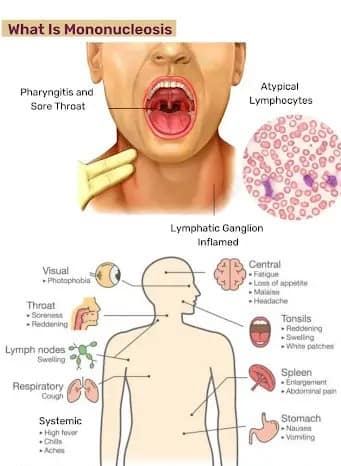
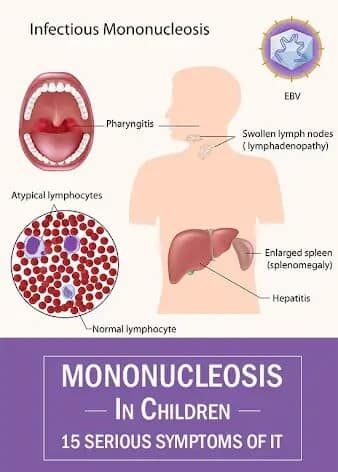
What is infectious mononucleosis?
Infectious mononucleosis is caused by the Epstein Barr virus that affects teenagers and adults. These viruses can spread through semen during sexual intercourse, organ transplantation, and blood. These viruses can be detected in the saliva of people who don’t experience clinical symptoms. Even after recovery, the EBV virus can be detected in the blood cells and throat throughout life. It has been estimated that around 95% of individuals get the infection by the age of 35.
Clinical symptoms:
- Enlargement of spleen
- Sore throat
- Extreme tiredness
- Skin rashes
Diagnosis:
Clinically, the healthcare professionals will check for swollen lymph nodes in the neck region. The presence of certain white blood cells (atypical lymphocytes) can indicate infection. Antibodies can be detected against the EBV or cytomegalovirus, which are formed in response to infection.

Heterophile antibody test (Monospot test) is another diagnostic method that can be used for detecting infectious mononucleosis The positive results can confirm the disease. If the individual has another health condition, the test can become falsely positive.
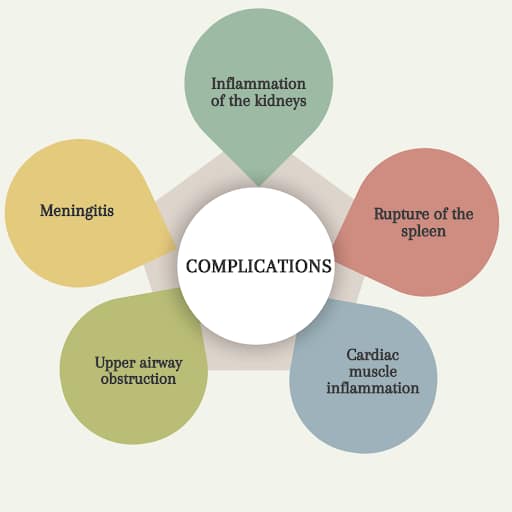
If left untreated, there can be several complications, such as
- Inflammation of the kidneys
- Rupture of the spleen
- Cardiac muscle inflammation
- Upper airway obstruction
- Meningitis
Treatment strategies:
Anti-inflammatory medicines and antipyretics can be used to treat fatigue, sore throat, and fever. Generally, corticosteroids are not preferred due to immunosuppression. Nutritional intake, proper rest, and hydration are important to manage the condition. Sometimes, maculopapular rashes can develop in individuals who have taken antibiotics.
How to prevent the spread of infectious mononucleosis?
- Avoid close contact with infected individuals, as the virus can be transmitted through kissing
- Maintain a proper hygiene by regularly washing the hands with water and an antibacterial soap. Cover the mouth while sneezing.
- Don’t share personal items, cosmetics, utensils, or glasses.
- It is important to create awareness about the Epstein-Barr virus, particularly among teenagers.
What are the overlapping clinical symptoms that exist between Lyme disease and infectious mononucleosis?
The diagnosis can be challenging due to overlapping clinical symptoms, particularly in the early stages. Key overlapping symptoms include,
- Extreme fatigue that persists for weeks or several months
- Mild or moderate grade feverSwelling of lymph nodes
- Musculoskeletal pain
- Rashes can develop in infectious mononucleosis, particularly after antibiotic use. Characteristic bull’s eye rashes or erythema migrans can occur in Lyme disease.
Case studies:
A 5-year old boy was experiencing intermittent fever, fatigue, abdominal pain, etc. On clinical examination, there was throat erythema. There were no skin rashes or hepatosplenomegaly. There was no history of tick bite. Serology tests (Enzyme-linked immunosorbent assay and IgM immunoblot) were found positive.
The patient also developed erythema migrans rashes that indicated early disseminated Lyme disease. After confirming the diagnosis, 14 days of antibiotic therapy were initiated. With antibiotic treatment, clinical symptoms resolved, which contributed to a better prognosis.
An 8-year old boy was experiencing sore throat and joint pain. The pain was radiating to the left ankle and wrist. The patient didn’t have a history of tick bite. The test results were negative for heterophile antibodies and Group A Streptococcus pharyngitis.
Both ELISA and Western immunoblot tests were positive. Initially, the clinical symptoms worsened after starting amoxicillin. Ultrasound confirmed the enlargement of the spleen and lymphadenopathy. Repeated tests revealed seroconversion. There was complete recovery after the administration of 21 days of antibiotics. Hence, Lyme disease was confirmed in both cases.
How to differentiate infectious mononucleosis from Lyme disease?
Exposure history serves as one of the distinguishing factors. Lyme disease is spread by tick bites, whereas infectious mononucleosis is spread through oropharyngeal secretions. Clinical features of infectious mononucleosis include enlargement of the tonsils, sore throat, etc. However, Lyme disease presents with bull’s eye rashes. Neurological manifestations (meningitis) can develop in later stages of Lyme disease.
Laboratory tests can provide better clarity. Lyme disease can be confirmed with the help of Enzyme Linked Immunosorbent Assay (ELISA), Western blot, polymerase chain reaction (PCR), etc. Infectious mononucleosis can be confirmed using heterophile antibody tests. Hence, a careful analysis of clinical symptoms, exposure history, and diagnostic tests can help to differentiate both the conditions.
What are the recommendations for physical activity in patients recovering from both Lyme disease and infectious mononucleosis?
Both Lyme disease and infectious mononucleosis require proper monitoring to manage the clinical symptoms. When these two conditions occur simultaneously, the symptoms can aggravate.
Adequate sleep must be ensured to enhance the chances of recovery. High-intensity workouts must be avoided for proper stabilization of health status. Patients should start with light activities, such as walking. A multidisciplinary approach from various specialists can guide the recovery of the patients.
How to prevent Lyme disease?
- While you are performing an outdoor activity, protective clothing (long sleeves, pants and shoes) should be worn.
- Wearing light-colored clothes helps to detect ticks. The use of tick repellents (DEET/permethrin) can greatly decrease the risk of tick bites.
- Taking a bath after an outdoor activity can remove the unattached ticks.
- Tweezers can be used to remove the ticks by holding them with slight pressure. The ticks must be removed within 24 hours to reduce the chances of infection.
Conclusion
- Both Lyme disease and infectious mononucleosis are infectious conditions with distinct etiologies.
- Overlapping clinical symptoms can make the diagnosis complicated, which contributes to delayed treatment.
- It is important to differentiate the two conditions at an early stage to ensure effective care.
Are you ready to take the next step towards your healing journey?
References
- Johns Hopkins Medicine. Infectious Mononucleosis [Internet]. Baltimore (MD): Johns Hopkins Medicine; [cited 2025 Jul 17]. Available from: Click Here
- Cleveland Clinic. Mononucleosis (Mono) [Internet]. Cleveland (OH): Cleveland Clinic; [cited 2025 Jul 17]. Available from: Check Now
- Mohseni M, Boniface MP, Graham C. Mononucleosis [Internet]. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025 Jan– [updated 2023 Aug 8; cited 2025 Jul 17]. Available Here
- Koester TM, Meece JK, Fritsche TR, Frost HM. Infectious mononucleosis and Lyme disease as confounding diagnoses: a report of 2 cases. Clin Med Res. 2018 Dec;16(3‑4):66–68. doi:10.3121/cmr.2018.1419. PMID: 30166498; PMCID: PMC6306145 [cited 2025 Jul 17].
